Why Go to Medical School? Reason #2

There's been a fair amount written about the true cost of medical school. A quick survey includes:
1) quarter of a million dollars, down the crapper.
2) 4 years for the privilege of losing another 3-5 years
3) previous relationship
4) previous waist (3 and 4 may be related)
5) all previous hobbies and interests
6) ability to have non-medical conversations (throw this in with 3 and 4)
And we slug it out, each of us, for the dream of becoming competent. I find little solace living with the knowledge that everything I have learned I will likely forget, and that everything I really NEED to know I won't see until years 3, 4, or beyond. Ergo: nothing I am learning now is making me competent. Makes it hard to give a GODDAMN about osteomalacia.
So I'm fighting back. I'm going to save each and every person out there from doing this for the wrong reasons. How, you ask? I am going to start posting here all of the useful things that I am learning in medical school. Things that will change your life, every day. After reading these, the best medical gems, do you still want to come learn the boring stuff?
This is the first installment:
Working Title: Reason #2
Alternate Title: The Grace of Defecation.
First, let's start with a little Anatomy. You're a tube with limbs. You're mouth is connected directly to your anus. Along the way it bubbles and flares into your stomach, small intestine and large intestine. Your large intestine is also known as the "colon." I didn't know that before coming to med school, and thought the colon was it's own organ just like the mysterious "prostate," which I thought meant "lying down."
Everything you eat is slowly sucked dry of the nutrition and turned into waste. It's this sloppy green paste that's found in the small intestine. Then the colon takes over and the magic begins. The colon sucks the paste dry and ages it, like the worst wine imaginable, into a brown solid. The colon fills with this and stores it until it's convenient to void it, and aren't you glad for that small courtesy?
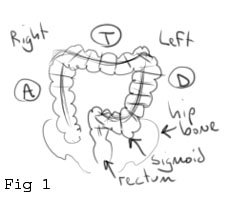
This is my drawing of the colon (Fig. 1). It bubbles and squeezes and pushes the waste through the Ascending Colon on the right, it travels along the upper deck of the Transverse Colon, and then it slides on down the Descending Colon. You'll notice that the Descending Colon is a little "off aim" from the rectum, that is, it isn't a straight shot. That connecting segment is the Sigmoid (S-shaped) Colon and its little kink is the life-saver. Without that, it would be much more difficult to restrain your bowel movement (BM). At last, we have the anal sphincters. You didn't know there were two, did you? Yup, the inner sphincter is under your body's control. Like any Control Tower, it doesn't let anything take off until it sees a need. The outer anal sphincter is under your conscious control and has to wait for ground clearance. Once that clearance is granted, it's the pilot's decision for go/no-go.
Now let's talk technique. The pressure of building feces is usually enough to have the BM. Untrained children know this. That's not why you're reading this. You're reading this because you are a professional, and professionals keep current with the latest journals. In the event that you have passed the golden two minutes and are losing hope for this BM, there are tricks both mechanical and chemical.
Mechanical: Remember Fig. 1? Like any hand-held maze with a single marble, the trick is to coax the feces down the chute. The order is crucial. First, lean hard to your left (Fig. 2). This ensures that any marbles in the upper deck are packed into the Descending Colon. Hold that position, shake a little, use your best judgment. When you are satisfied, bank a hard right (Fig. 3). This maneuver will hopefully un-kink and straighten the Sigmoid Colon, ensuring a straight shot and maximum pressure against the Control-Tower-Sphincter. Hopefully, you get clearance.

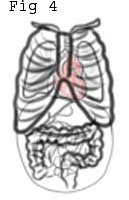
If this does not work, you have reserves. Your abdomen is filled with your guts and sits below your lungs and heart (Fig. 4). Your abdomen is also shrink-wrapped in muscles. Both can be used to advantage. Most everyone knows that crunching up your abs and leaning forward helps. Both moves compress the abdomen and build up pressure. But without incorporating the lungs, it's like throwing a fist flat-footed. You've GOT to put your weight behind that punch! You do this using the Valsalva maneuver. It was originally developed to help push pus out of the ear. We're going to modify it.

Because you're chest is next to your abdomen, building up pressure in one builds pressure in the other. That's why a punch in the stomach (increase in abdominal pressure) knocks the wind out of you. That's why building pressure in your chest is going to knock the poop out of you. To build up pressure in your chest, take a deep breath, close your throat (or pinch your mouth and nose), and SQUEEZE! Try to forcibly exhale against your closed throat, press your elbows against your sides, crunch your abs and lean to the right. If you'd rather use a more familiar tack: blow your nose (Fig 5). Hopefully, your best efforts will bear fruit.
That was graphic, right? Now that we're done with mechanical, let's talk chemical. Certain foods help us void. I remember the first time in my life when something was "stuck" in there. My father brought me a bowl of Cheerios. I was six years old and didn't know any better. While fiber and other ruffage (think leafy greens) helps keep us regular, it's more preventative than curative. For the right here and right now, you'll need some caffeine. Caffeine is a stimulant and a diuretic (makes our urine clear). Clears the mind; sharpens the senses. It also accelerates the colon's normal shuffling action. Unfortunately, our coffee mugs are usually out of reach, and it's a little embarassing to call a coworker or family member for a cup. I'll never forget the time I ran out of toilet paper at a friend's house. "There's more underneath the sink!," he yelled. I leaned over to throw the door open and there, next to a fresh role of Downy, was a single can of RedBull. This was a man who knew what he was doing. I've kept an emergency can by my thrown ever since.

So that's my advice. Rock left, then right. Blow your nose. Have an emergency can of Red Bull. I just saved you $45,000.
Having read this, I know that each of you is thinking: "What is wrong with this person? Who sits down to write a manifesto on the bowel? With pictures? I can't believe I just spent 5 minutes reading that." To which I respond, "Try, just try, to forget it. Also, you're welcome."
Disclaimer: I have not conducted barium studies to verify my shuffling bowel theory. I am not a nutritionist or a gastroenterologist.
posted by M. Dyspnea @ 7:37 PM
5 comments
![]()
![]()



5 Comments:
If you had posted an email address, I'd send this to you directly, rather than risk criticism for hyping my book. But since there are no other comments, this is close to a private conversation. So let me respond to a post of yours on Respectful Insolence.
First, I'm a nearly-retired general surgeon. I trained at a very academically oriented program (UCSF, in the 1970s). Most of my training-mates are in academic surgery. I spent my career in private practice. I can tell you neither is perfect. I think it's very safe to say private practice is much more time-consuming, especially after hours. The day Orac described as especially gruelling was like it was for me very often during my career of being on call every third night and every third weekend. That he spent only one night up during a three-day weekend was a piece of cake! Also, note that he got the call after the resident had spent hours (perhaps) doing the evaluations that a private practicing surgeon would have been doing him- or herself. So clearly, they get more sleep. In my practice, I'd never have the time to blog the way Orac does (compare the frequency of posts on the blog of a private surgeon, "A chance to cut is a chance to cure."
Academics have to contend with grants, departmental politics, diminishing reimbursement as it affects teaching. On the other hand, they do get to teach -- which I missed -- and do research which is presumably a love and is therefore fulfilling.
I think the greatest reward of private practice is the intimacy of the relationship with the patient. It's removed a bit in academe, as filtered through resident staff. The greatest reward of academe, as far as I can see from my friends in the field, is the ability to push the field forward.
Finally, the part I could get criticized for: if you're interested in surgical training, I think you'd find my book enlightening, as well as entertaining. It's called "Cutting Remarks; insights and recollections of a surgeon." It's about my surgical training. You can find it at the usual places online and elsewhere. Good luck with your choice of medicine as a career.
...and can i just say that your writing continues to kill me.
a "medical" book more in line with your personality and style, i think, would be frank vertosick's "When the Air Hits Your Brain:Tales of Neurosurgery." a funny book.
Nice blog. I will keep reading. Please take the time to visit my blog about loss weight program
I just spent the last 2 hours searching every blog and website struggling to figure out whether medicine is worth all its woes. While your blog didn't help in my decision at all (although I can say I am dying to learn more of these "fun" facts), I was compelled enough to leave my first ever comment on a blog. I laughed throughout, especially hard when I found myself attempting each of your proposed techniques as I read. Thanks for the humor. I needed it. Looking forward to your book!?
Real nice job! Good stuff here. Doesn't This looks like an awesome place to begin your academic program! The True Blue Campus at St. Georges University.
Post a Comment
<< Home