I do not care much for scare tactics. It is a right of passage in high school that a local police officer comes before the entire student body to give a lecture on the dangers of drunk driving. I remember hearing about it beforehand that this guy used scare tactics and would show us a bunch of car crashes that claimed the lives of teens 'just like you'. Most of my friends thought, “Cool! I like car wrecks. Let's see who totaled his car the worst.” Slide after slide of cars bent around trees, charred from fires and road scenes cleared of everything except a little blood on the asphalt clicked by. We would snicker to each other, “Wow, that guy must have been going fast.” Sure, we were being callous on purpose, but the consequences just couldn't register anyway. Then he brought out the beer goggles.
These were thick plastic lenses that horribly distorted your vision. He lectured us about the level of alcohol in your system after a single beer, and how you were drunk after just two.
Don't believe me? I'll show you what it's like for someone your age after two beers He asked someone to come onto the stage to wear the goggles, and he would let us all laugh at our friend's inability to walk against his best efforts to just ‘maintain’. That’s when the officer would yell sternly, “That’s what it’s like when you’re drunk! Not funny, is it!” What a bag of mixed messages.
Presentation style aside, we didn’t take him seriously because we knew the magician’s trick. We had all been drunk and, from that, we all knew that those goggles were far from our experience. Inebriation after two beers was far from our experience. His mistake was trying to shock and scare us into doing the right thing when giving us the information about alcohol's effects and trusting us to make the right decision might have worked. After all, regardless of what is said in a lecture hall, the decision was going to be ours.
The reason I am relating this: it was not until I was in medical school that I was given all of the information about alcohol that would have been so useful then. Though I long ago recognized the unacceptable risk of driving drunk, it’s only now that my decision feels informed. I do not see why this moment has to come $100,000 later, eight years out of high school. Worse, I recognize that very few people are ever in this position to learn it.
I'm going to try over the next few weeks to lay out everything that I have learned in the past two years that has helped me reconcile my experience with alcohol with the science of alcohol. I want the person interested to understand the greater story of how our body and brain interact with alcohol, why understanding it is exciting in and of itself, and how knowing all of this might help you put your own experiences into a context more helpful than a car crash.
It is my hope that you can make the decision yourself, informed.
***
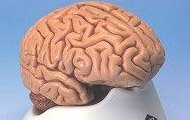
The brain is divided both in shape and in function. In shape, we are used to thinking of a left brain and a right brain, but the biggest differences are between higher and lower function. The classic picture of the brain is of the mess of infoldings that is split down the middle. This is your cerebral cortex with its left and right hemispheres. The highest of your thoughts live here. Pronouncing a word, telling a joke with the right emphasis, drawing a picture; all of it is happening somewhere inside those folds. Not every spot is created equally: some of the areas in your cortex are incredibly important (being able to speak) while others are less important. For example: Phineas Gage. The most famous survivor of brain damage, Phineas was a railroad worker who accidentally triggered an explosion that sent a railroad spike through his cheek, left eye, and into his brain. The only thing that changed was his personality. James Shreeve writes “[i]n place of the diligent, dependable worker stood a foulmouthed and ill-mannered liar given to extravagant schemes that were never followed through. ‘Gage’, said his friends, ‘was no longer Gage’.” Even so, he was still alive and functioning.
It is hard to understate how incredible an idea this is. There are parts of our brain that, should they go missing, we may never care. There are parts of our brain that when damaged, merely change aspects of our personality. Remove the entire brain and we certainly die. Exactly how much of the brain could be whittled away before we could no longer live? What parts are essential to life and what is going on there?
***
Why do we drink? I am not trying to be philosophical, but I am trying to reduce the urge to what it is: it pleases us. We drink in celebration, to lower inhibitions, to blunt depression, to satisfy addiction. The ways in which alcohol is used and abused are not important for the discussion here, but I do want you to appreciate how powerful a motivator our own pleasure can be.
In the 1950s, two scientists performed a famous experiment on rats. To map the brain (even now in neurosurgery) the physician will electrically stimulate an area and test for the expected response. Imagine a patient awake, with his brain open to the air, as a surgeon electrically disrupts certain areas looking for the portion of the brain that stores “mammals”, for example.
“Okay Jimmy, I want you to name every mammal you can think of.”
“Elephant, dolphin, tiger, ...daaaaaa”
“Got it!”
Today’s neurosurgeon benefits from a rough map of the brain that has been established over years of investigations. But what if you didn’t have even a rough idea? What if you were back in the 1950s? Peter Milner and James Olds decided to poke around.
They experimented by implanting electrodes into the brains of rats, electrocuting them, and watching for the effects. They found that with a certain placement, the rats appeared to experience ecstasy on stimulation. Had they found the rumored “pleasure center”? Next, they introduced a lever into the cage that the rat could press at will to send a stimulus directly to its brain. What they found was disturbing: the rats would press the lever 2,000+ times an HOUR. They rats wanted it more than food and water. They would press it until they died.
***This post will be completed at my new home,
The rumors were true